Introduction: For half a century, a high level of total cholesterol (TC) or low-density lipoprotein cholesterol (LDL-C) has been considered to be the major cause of atherosclerosis and cardiovascular disease (CVD), and statin treatment has been widely promoted for cardiovascular prevention. However, there is an increasing understanding that the mechanisms are more complicated and that statin treatment, in particular when used as primary prevention, is of doubtful benefit.
Areas covered: The authors of three large reviews recently published by statin advocates have attempted to validate the current dogma. This article delineates the serious errors in these three reviews as well as other obvious falsifications of the cholesterol hypothesis.
Expert commentary: Our search for falsifications of the cholesterol hypothesis confirms that it is unable to satisfy any of the Bradford Hill criteria for causality and that the conclusions of the authors of the three reviews are based on misleading statistics, exclusion of unsuccessful trials and by ignoring numerous contradictory observations.
Full Paper: https://doi.org/10.1080/17512433.2018.1519391
Okay, I've been happily ignoring your little idee fixee on LDL aside from one gentle comment but I feel the need to comment here again.
This article is utterly disingenuous and sets up a complete strawman to knock down. It sets out to disprove a notion of cholesterol that was last current decades ago. Right in the first paragraph and throughout the article LDL is referred to as “the” major cause of atherosclerosis which to my knowledge even the Framingham authors wouldn't have been comfortable with, it is however a significant contributing factor.
It is well known that some people with elevated LDL or total cholesterol are at low risk(this is the reason for weak or negative results in whole population studies), atherosclerosis is a complex disease with multifactorial causes, no practising doctor I know thinks it is “the” major cause, or even the most important contributing factor.
That being said it is thoroughly established that statin use in select patients reduces the risk of MI and CVA, especially in those with established atherosclerosis, but also those with other substantial risk factors (high BP, family history, smoking, diabetes etc.). This is totally uncontroversial and the pathogenic mechanisms, while complex, are increasingly well understood.
I have been a doctor for over a decade and I consider myself diligent in keeping up with research, and although the selection of patients for statin therapy is an ongoing and regularly changing area of research on which experts can disagree, the fact that select patients will have substantially lower risk of coronary events due to statin therapy is uncontroversial.
Here is an article written by people who payed attention in stats class and have bothered to make their case with evidence rather than knocking down strawmen
Efficacy and safety of long-term treatment with statins for coronary heart disease: A Bayesian network meta-analysis (2016)
Or for a more succinct and easy to read summary here is the Cochrane conclusion
"Of 1000 people treated with a statin for five years, 18 would avoid a major CVD event which compares well with other treatments used for preventing cardiovascular disease."
Statins for the primary prevention of cardiovascular disease
Great phrase! new to me, I had to look it up. For what it's worth, I don't have any personal investment in the LDL debate. My LDL falls in the recommended guideline ranges anyway. https://hackertalks.com/post/6749910
I'm just curious.
I think your statements and the paper are congruous. The target audience for the paper are the people who treat LDL in isolation.
It does appear that Targher et al do agree with your concerns of the paper: https://doi.org/10.1080/17512433.2019.1561100
My understanding of Ravnskov's commentary in the LDL-C paper is not that statins have no value in all circumstances, but that diet and lifestyle treatments (he implies, but does not say explicitly) would have more impact in isolation then statins in isolation especially in contexts where LDL is the only presenting risk factor.
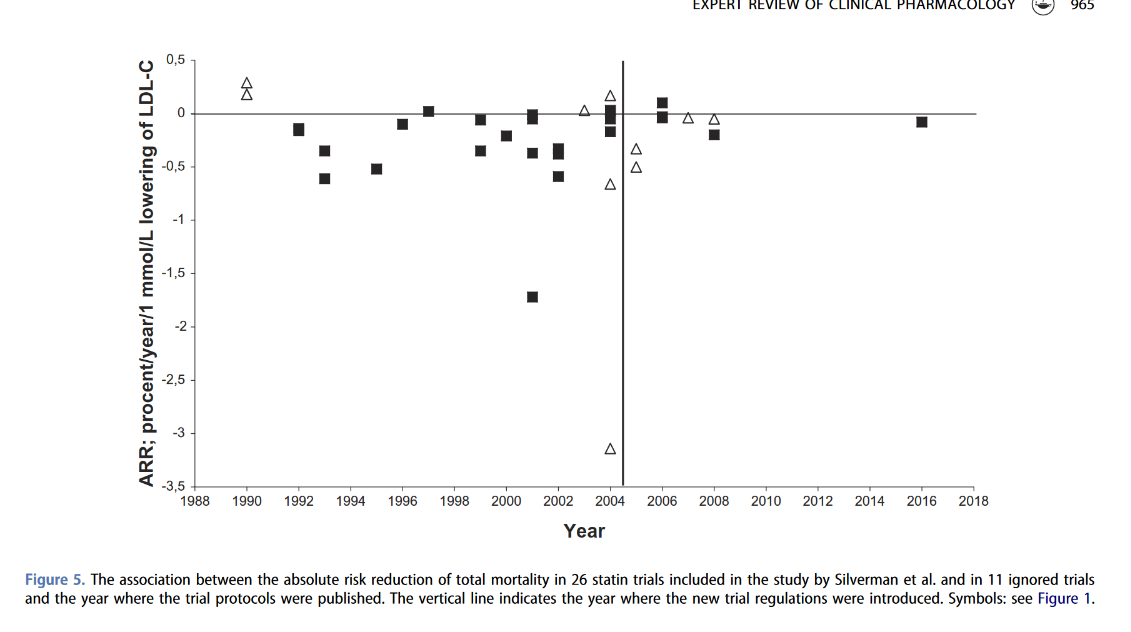
Ravnskov does state that there is a significant relative risk reduction with a statin, but the absolute risk reduction isn't significant. Ravnskov's commentary about the pre-study washout skewing results would apply to the meta-analysis and Cochrane review below
I couldn't get access to the supplement section to see the list of studies included to compare against Ravnskovs included studies, but the papers mortality numbers are all presented in RR terms.
It appears that only RR is computed.
Ravnskov does include many of the studies from Figure 1.
This is also a major point Ravnskov makes.
I really appreciate you reading the paper and giving us your analysis. This is exactly why I come to lemmy.
I suppose Ravnskov's new opinion on the EU CVD guidelines would also not be viewed favorably? https://doi.org/10.1080/17512433.2020.1841635
As far as I'm aware there is no analysis of statins on a healthy adult population, it would be interesting to see. https://doi.org/10.3390/medicina57060585