Introduction: For half a century, a high level of total cholesterol (TC) or low-density lipoprotein cholesterol (LDL-C) has been considered to be the major cause of atherosclerosis and cardiovascular disease (CVD), and statin treatment has been widely promoted for cardiovascular prevention. However, there is an increasing understanding that the mechanisms are more complicated and that statin treatment, in particular when used as primary prevention, is of doubtful benefit.
Areas covered: The authors of three large reviews recently published by statin advocates have attempted to validate the current dogma. This article delineates the serious errors in these three reviews as well as other obvious falsifications of the cholesterol hypothesis.
Expert commentary: Our search for falsifications of the cholesterol hypothesis confirms that it is unable to satisfy any of the Bradford Hill criteria for causality and that the conclusions of the authors of the three reviews are based on misleading statistics, exclusion of unsuccessful trials and by ignoring numerous contradictory observations.
Full Paper: https://doi.org/10.1080/17512433.2018.1519391
This is a very easy to read paper, I highly recommend skimming it at least.
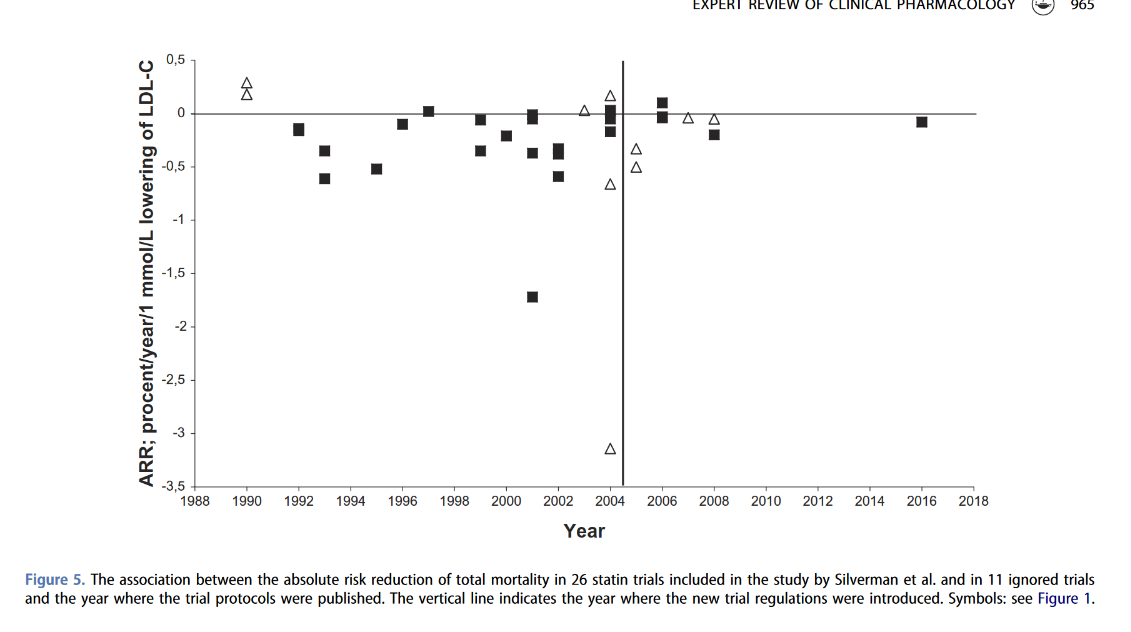
TLDR: Academic fraud pushing an agenda, unpublished results, and the immense lack of papers since the new trial protocols were required (i.e. must register, must publish, can't ignore bad results)
exposing academic fraud and data manipulation
Taking a medicine for life to pull down a ldl metric that causes many issues (t2d, insulin resistance)... for a few extra days of life?.... this is why they never report absolute risk reduction
Shouldn't this show up in all cause mortality data? or this effect is beyond the study length?
That is interesting, high LDL is protective against cancer, if you only treat people with high LDL you can show a benefit from cancer compared to a general population.....