Friendly Carnivore
82 readers
1 users here now
Carnivore
The ultimate, zero carb, elimination diet
Meat Heals.
We are focused on health and lifestyle while trying to eat zero carb bioavailable foods.
Keep being AWESOME
We welcome engaged, polite, and logical debates and questions of any type
Purpose
- lifestyle
- food
- Science
- problems
- Recipes
- Sustainability
- Regenerative lifestyle
Rules
- Be nice
- Stay on topic
- Don't farm rage
- Be respectful of other diets, choices, lifestyles!!!!
- No Blanket down voting - If you only come to this community to downvote its the wrong community for you
- No LLM generated posts . Don't represent machine output as your own, and don't use machines to burn human response time.
Other terms: LCHF Carnivore, Keto Carnivore, Ketogenic Carnivore, Low Carb Carnivore, Zero Carb Carnivore, Animal Based Diet, Animal Sourced Foods
Meta
If you need to block this community and the UI won't let you, go to settings -> blocks you can add it.
[Meta] Moderation Policy for Niche Communities
founded 4 months ago
MODERATORS
1
Carnivore Resources
YouTube Carnivore
Science Based, Factual Discussions:
Experience, testimonials:
Nutritionists/Coaches:
Lifestyle/Influencers:
Mini-Series on all aspects of the Meat science, heath, nutrition, and environment
Books Carnivore
Websites Carnivore
Excellent resource with many references on all things carnivore, may have to click around, recommend
Ketogenic Resources
Carnivore is a subset of Ketogenic eating, so all of the benefits for keto also apply here
YouTube Ketogenic
Science Based, Lectures:
Websites Ketogenic
Science, Guides, Recipes , Hard Science, highly recommended
Keto Virtual Health Program - monitoring, medication titration, coaching, excellent
Books Ketogenic
- Ketogenic : The Science of Therapeutic Carbohydrate Restriction in Human Health
- Why We Get Sick: The Hidden Epidemic at the Root of Most Chronic Disease--and How to Fight It
- How Not to Get Sick: A Cookbook and Guide to Prevent and Reverse Insulin Resistance, Lose Weight, and Fight Chronic Disease
Feel free to add any suggestions below.

2
- Red meat is a nutrient dense food providing important amounts of protein, essential amino acids, vitamins, and minerals that are the most common nutrient shortages in the world, including vitamin A, iron, and zinc.
- Despite claims by the World Health Organization (WHO) that eating processed meat causes colon cancer and red meat probably causes cancer, the observational data used to support the claims are weak, confounded by multiple unmeasured factors, and not supported by other types of research needed for such a conclusion. Although intervention studies are designed to test the validity of associations found in observational studies, two interventions of low-fat, low-meat diets in volunteers that failed to find a benefit on cancer were not considered in the WHO decision.
- It is likely that the association of red-meat consumption with colon cancer is explained either by an inability of epidemiology to detect such a small risk or by combinations of other factors such as greater overweight, less exercise, lower vegetable or dietary fiber intake, and perhaps other habits that differentiate those who eat the most meat from those who eat the least.
Full Paper - https://doi.org/10.1093/af/vfy009

3
4
5
Cancer as a metabolic disease
The big fat surprise
Why we get sick
How not to get sick
Some nice physical reading ahead
6
7
10
11
12
13
14
15
Loved the pictures of all the breeds of cow and also the description of how they've come about and what they taste like. I personally don't actually like A5 Wagyu that much, but plain old Japanese beef and not Wagyu I like a lot.
The colour of the fat showing how nutritious it is (yellow = grass fed) is a nice bit of knowledge to have! I'd also love to be able to dry age my own beef, but I think that's quite an endeavour. Would make a nice project to do on the side, maybe.
::: spoiler Results

16
17
18
19
20
21
So the official place to get it requires a login: https://doi.org/10.1016/S0140-6736(25)01201-2
But the full report can be found on : https://www.donorplatform.org/wp-content/uploads/2025/10/PIIS0140673625012012.pdf
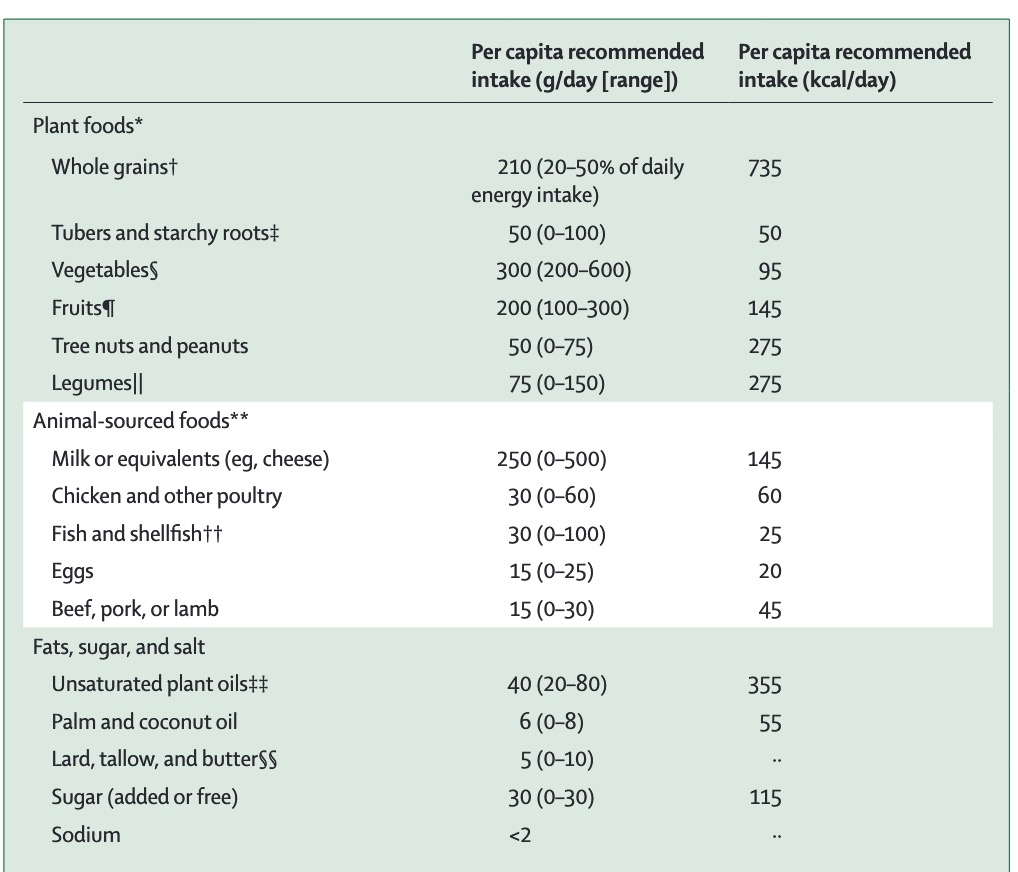
I'll summarize:
60% Carbs, 20% protein, 20% fat
Highly processed seed oils and highly processed grains are the major source of energy on this diet.
Obviously this is counter to the health goals of keto/carnivore, but it's remarkable here as this will be used to drive lots of anti-meat efforts globally, so its good to become familiar with it.
22
23
24
25
view more: next ›